전문가가 아닌 환자들의 치료에 참고가 되도록 논문을 소개해 본다.
The recurrence and survival of oral squamous cell carcinoma: a report of 275 cases
Abstract
Oral squamous cell carcinoma (OSCC) is a common malignant tumor of the head and neck, and recurrence is an important prognostic factor in patients with OSCC. We explored the factors associated with recurrence of OSCC and analyzed the survival of patients after recurrence. Clinicopathologic and follow-up data of 275 patients with OSCC treated by surgery in the Cancer Institute and Hospital of Tianjin Medical University between 2002 and 2006 were analyzed. Recurrence factors were analyzed with Chi-square or Fisher’s exact test and multivariate analysis. The prognosis of patients after recurrence was analyzed with the Kaplan-Meier method and log-rank test. The recurrence rate was 32.7%. The recurrence time ranged from 2 to 96 months, with a median of 14 months. Univariate analysis showed that T stage, degree of differentiation, pN stage, flap application, resection margin, and lymphovascular invasion were factors of recurrence (P < 0.05). Multivariate analysis showed that T stage, degree of differentiation, and pN stage were independent factors of recurrence (P < 0.001).
구강의 편평상피암은 흔한 두경부의 악성 종양으로, 재발율은 중요한 예후를 측정할 수 있는 요인이 된다. 우리는 구강암의 재발에 관한 요인을 탐구하여서 재발 뒤의 생존율을 분석하였다. 임상 병리적 연구 와 함께 생존율을 측정하였는데 이 데이타는 천진의학대학에서 2002년부터 2006년까지 수술을 받았던 275명의 환자에 관한 통계이다. 재발 뒤의 환자의 예후를 분석하는 데는 카프란메이어 생존율 분석법과 로그랭크 테스트를 이용하였다. 재발율은 32.7%였다. 그리고 재발의 시간은 2개월부터 96개월(8년)까지 있었다. 평균적으로는 14개월만에 재발을 하였다고 볼 수 있다. 단변량분석법에 의하면, T stage(종양의 크기)와 분화도, pN stage(림프절 전이여부), flap application(치근막에 수술에서의 방법), resection margin (절제선의 침범여부), 그리고 혈관림프절의 침범 등이 재발의 요인에 관여하였다.
The differences in gender, age, tumor site, region of lymph node metastasis, and perineural invasion between the recurrence and non-recurrence groups were not significant (P > 0.05). Kaplan-Meier and log-rank tests showed that the 2- and 5-year survival rates were significantly lower in the recurrence group than in non-recurrence group (67.6% vs. 88.0%, 31.8% vs. 79.9%, P < 0.001). Therefore, to improve prognosis, we recommend extended local excision, flap, radical neck dissection, and adjuvant chemoradiotherapy for patients more likely to undergo recurrence.
성별과 나이 종양의 부위 림프절 전이 부위와 신경침윤(perineural invasion)의 정도는 재발한 그릅과 재발하지 않은 그룹 사이에 별 중요한 차이를 보이지 못했다. 카플란마이어 생존율 방법을 이용한 결과 재발한 그룹에서는 재발하지 않은 그룹 사이에서 2년과 5년째에 많은 차이가 있었다(2년째는 재발집단에서는 67.6 %를 보이는 반면에 비재발집단에서는 88% 생존율을 보였고, 5년째에는 31.8%와 79.9% 로 차이가 보였다). 그러므로 좋은 치료 예후를 위해서 우리는 광범위한 국소절제술과 판수술,경부림프절 절제와 보완적인 화학치료를 재발율이 높은 그룹에 권한다.
Incidence of head and neck cancer is approximately 14/100,000, accounting for 16% to 40% of all malignancies. Oral squamous cell carcinoma (OSCC) is the most common malignant tumor of the head and neck, and its incidence has increased in recent years[1]. Surgery is the preferred treatment of OSCC. Despite great progress in chemotherapy, radiotherapy, and targeted therapy in the last three decades, the prognosis of OSCC is poor due to aggressive local invasion and metastasis, leading to recurrence. Thus, OSCC is still a challenging disease to treat in the field of head and neck cancer. Recurrence is an important prognostic factor in patients with OSCC. Camisasca et al.[2] have reported that the 5-year survival rate was 92% in OSCC patients without recurrence and 30% in patients with recurrence (P < 0.001, log-rank test). The median survival was 76.8 months in patients without recurrence and 42.5 months in patients with recurrence (P < 0.001, log-rank test). Lindenblatt et al.[3] have reported that recurrence affected the 5-year survival rate and disease-free survival of patients with OSCC. Postoperative tumor recurrence leads to a poor prognosis and a poor quality of life. Identifying factors that affect the recurrence of OSCC to reduce postoperative recurrence is an emerging issue in clinic.
두경부암의 발병율은 대략 10만명 중의 14명이다. 그리고 16-40%가 악성이다. 구강의 편평상피암은 두경부암 중에 가장 흔한 악성종양으로 최근에 발병율이 증가추세에 있다. 수술이 권고되는 치료방법이다. 화학치료나 방사선치료 표적치료 등의 놀라운 진전에도 불구하고 구강의 편평상피암의 예후는 매우 좋지 않다. 왜냐하면 공격적인 국소 침범과 전이가 재발을 유도하기 때문이다. 그러므로 구강암은 여전히 두경부암의 영역에서 치료에 많은 도전이 필요한 영역이다. 재발이란 구강암환자에게서 매우 중요한 예후를 예측할 수 있는 요소이다. camisasca etal-의 리포트에 의하면 재발을 안한 경우는 5년 생존율이 92%에 달하지만 재발한 경우는 5년 생존율이 30%에 불과하다 .
또한 중앙생존기간은 재발하지 않은 그룹은 76.8개월(6년 4개월)인 반면에 재발한 환자의 그룹에서는 42.5개월(3년 6.5개월)이었다. Lindenblattet al의 보고서에 의하면 발이 5년 생존율과 무병생존율에 영향을 준다고 하였다. 수술 후에 재발은 나쁜 예후를 보여주고 삶의 질에서도 매우 나쁘다. 그리하여 재발에 영향을 주는 요소를 찾아내는 것이 임상상 떠오르는 이슈가 된다.
이하 문장에서 중요한 이해를 돕기 위해 필요한 부분만을 일반인을 위해서 번역을 해 보겠다.
In this study, we collected clinicopathologic and follow-up data of patients with OSCC and analyzed recurrence factors and patient survival. Our study provides a basis to develop standardized treatment protocols for OSCC.
Materials and Methods
Patients
All patients were treated at Tianjin Medical University Cancer Hospital between January 2002 and December 2006. Patient inclusion criteria included the following: (1) all patients were first treated, (2) all patients underwent surgery, (3) primary OSCC was confirmed by both preoperative and postoperative pathologic examination, and (4) complete clinicopathologic and follow-up data were available. Local recurrence, regional recurrence, or both were all defined as recurrence. Time to recurrence was determined by the duration from the first surgery to pathologically confirmed recurrence.
Treatment
Patients underwent surgery with other combined therapies. Patients at clinical stages I-II were treated with preoperative induction chemotherapy and surgery; patients at stages III-IV underwent preoperative chemotherapy, surgery, and postoperative radiotherapy or chemotherapy. TFP regimen was used for both preoperative and postoperative adjuvant chemotherapy: docetaxel at 60 mg/m2, day 1; cisplatin at 60 mg/m2, days 2 to 4; and 5-fluorouracil at 750 mg/m2, days 2 to 6.
환자들은 치료를 위하여서 수술과 다른 결합치료를 받았는데 임상적으로 1-2기 환자들은 수술 전 화학치료와 수술을 받았고 3-4 기의 환자들은 수술 전 화학치료와 수술 후에도 방사선치료 혹은 화학치료를 받았다. 그리고 TFP regimen이 수술 전이나 수술 후의 화학치료에 사용되었다.
이는 태음인약물인 docetaxel과 소음인 약물인 cisplatin과 역시 소음인 약물인 fluorouracil을 사용하는 방법이다. # 내개인 적인 견해로는 체질에 따라서 분리되어서 사용되면 훨씬 예후가 좋을 것으로 생각된다.
Simple primary tumor resection or extended tumor resection was performed according to tumor extent. For patients with poorly differentiated tumors at stages T3-T4, extended resection with a distance of at least 2 cm from the primary tumor was performed. Large wounds were repaired with skin flaps, such as the pectoralis major free flap, anterolateral thigh flap, fibular flap, and radial forearm flap. Selective neck dissection in the ipsilateral cervical I-III regions was performed for cN0 patients; radical neck dissection in the ipsilateral cervical I-V regions was performed for cN+patients. External beam radiation was used for radiotherapy. Patients with cervical recurrence and primary recurrence underwent rescue therapies, such as primary tumor resection, neck dissection, palliative chemotherapy, and radiotherapy.
Follow-up
Patients were followed up by hospital revisits, home visits, phone calls, or mails. The final date of follow-up was December 31, 2011. All patients were followed up for at least 5 years.
Statistical analysis
SPSS16.0 was used for statistical analysis. The relationships between clinicopathologic factors for OSCC and recurrence were analyzed using Chi-square or Fisher’s exact test. The Kaplan-Meier method and log-rank test were used for survival analysis. P < 0.05 was considered significant.
Results
General information
A total of 312 patients with OSCC were admitted between January 2002 and December 2006 to the Tianjin Medical University Cancer Hospital: 37 were lost to follow-up, and 275 met the inclusion criteria. The 275 patients ranged from 24 to 83 years old, with a median age of 58.5 years. The male to female ratio was approximately 1.9:1. Tongue cancer was the most common form of OSCC, followed by gingival cancer. Of the 275 cases, 214 were highly differentiated, 58 were moderately differentiated, and 3 were poorly differentiated. According to the 2002 UICC staging for OSCC, 75 cases were at stage T1, 107 at stage T2, 29 at stage T3, and 64 at stage T4; 103 had pathologically confirmed lymph node metastasis, and 172 did not (Table 1).
All patients underwent 2 cycles of preoperative neoadjuvant chemotherapy. Forty patients underwent postoperative radiotherapy with radiation doses of≥ 60 Gy for primary tumors,≥ 60 Gy for neck regions with lymph node invasion, and≥ 50 Gy for neck regions without lymph node invasion. Sixty-five patients underwent 1 to 4 cycles of postoperative adjuvant chemotherapy. Seventy-five underwent extended resection, and 62 had flap repair. Some patients abandoned treatment because of personal reasons.
모든 환자들은 2 cycle의 수술 전 화학치료를 받았다. 40명의 환자들은 수술 후에 60Gy 이상 용량의 방사선 치료를 원발 부위와 림프절 침범 부위에 받았고, 림프절 침범이 없는 경우는 50Gy 이상의 용량을 받았다. 65명의 환자들은 1-4 차례의 수술 후 화학치료를 받았고, 75명은 광범위한 절제술 그리고 62명은 판성형술을 받았다. 약간의 환자들은 개인적인 이유로 치료를 포기하였다.
Recurrence factors
Ninety (32.7%) patients had recurrence. Recurrence time ranged from 2 to 96 months, with a median time of 14 months. The tumor recurred in the neck in 45 patients, at the primary tumor site in 36 patients, and at both the primary site and neck in 9 patients. We performed univariate analysis between various clinicopathologic factors and OSCC recurrence. A lower recurrence rate was related with T1-T2 stage, well differentiation, pN0 stage, flap repair, negative tumor resection margin, and no extracapsular invasion (P < 0.05); gender, age, primary tumor site, regions of lymph node metastasis, and perineural invasion were not related to recurrence (P > 0.05) (Table 1).
32.7%의 환자가 재발을 하였고 2달부터 96개월에 걸쳐서 재발을 하였으며 중앙 재발기간은 14개월이다. 45명의 환자는 경부에 재발을 하였고 36명의 환자들은 원발 부위 즉 수술 부위에 재발을 하였고 경부와 수술 부위 양쪽에 재발을 한 경우는 9 경우이다.
Multivariate analysis showed that T stage, degree of differentiation, pN stage, and flap repair were associated with recurrence (P < 0.001) (Table 2).
Relapse-free survival
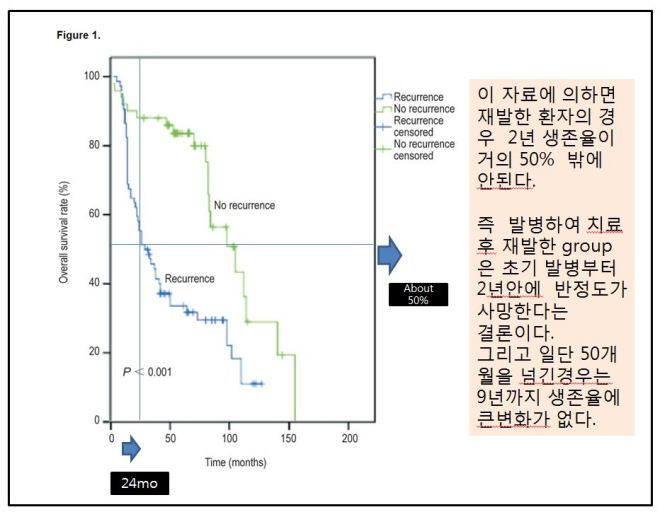
Seventy-two patients died due to tumor-related diseases, and 90 had recurrence. The 5-year overall survival rate was 54.5%. The survival time ranged from 6 to 120 months, with a median of 36 months. The Kaplan-Meier method and log-rank test showed that the 2- and 5-year survival rates were lower in patients with recurrence than in those without recurrence (67.6% vs. 88.0%, 31.8% vs. 79.9%, P < 0.001) (Figure 1).
72명의 환자들은 종양과 연관된 질환으로 사망하였고 90명은 재발을 보였다. 5년 생존율은 54.5% 였다. 생존기간은 6개월부터 120개월(12년)까지였고, 중앙 생존기간은 36개월(3년)이었다.

Discussion
In this study, 90 (32.7%) patients had recurrence. Chi-square or Fisher’s exact test and multivariate analysis showed that T stage, degree of differentiation, and pN stage were important factors of recurrence (P < 0.001). The 2- and 5-year survival rates were lower in patients with recurrence than in those without, as determined by the Kaplan-Meier method and log-rank test (P < 0.001).
이 연구에서 32.7% 에 해당하는 90명의 환자가 재발을 하였다. 그리고 T stage와 분화정도, 림프절 번이가 중요한 변수였다.
Factors that influence the recurrence of OSCC have been extensively explored in recent years. Ebrahimi et al.[4] have reported that T stage and N stage were important factors affecting regional recurrence in OSCC. Camisasca et al.[2] have analyzed patient clinicopathologic data, including tumor sites, clinical and pathologic stage, histological grade, invasion mode, and perineural invasion. They have concluded that tongue cancer and poor differentiation contributed to OSCC recurrence after surgery.
여러 가지 분석결과 혀에 발생한 구강암과 세포병리학에서의 poor differentiation이 구강암의 수술 뒤에 재발에서 높은 율을 차지한다.
Vázquez-Mahía et al.[5] have reported that the recurrence rate was 44.9% in 118 patients with OSCC. Statistical analysis showed that co-morbidities, degree of tumor differentiation, and tumor stage were important prognostic factors for recurrence. Using univariate Chi-square or Fisher’s exact test, we found that T stage, degree of tumor differentiation, pN stage, and flap repair were significantly related with tumor recurrence (P < 0.001). In our study, the recurrence rate was 32.7%, which was lower than the reported 35.5% to 47.1%[2],[4]. In the studies by Camisasca et al.[2] and Ebrahimi et al.[4], the patients underwent surgery only. Therefore, the lower recurrence rate in our study may be due to the following conditions: (1) preoperative 1-2 cycles of TPF neoadjuvant chemotherapy, (2) patients at advanced stages underwent postoperative 1-4 cycles of adjuvant chemotherapy or radiotherapy, or (3) complete tumor resection achieved with the help of various flaps. Therefore, we believe that T3-T4 stage, poor tumor differentiation, and pN positivity are important factors for the recurrence of OSCC. In addition, flap repair, adjuvant chemotherapy, or radiotherapy may also reduce recurrence.
우리의 연구에서 재발율은 32.7%로 기존의 35.5%나 47.1 %에 비해서 낮았다. 그리고 camisasca와 Ebrahii의 환자들은 수술만을 받은 환자들이었고, 자연 우리 연구에서 낮은 재발율의 요인은 다음과 같은 3가지로 본다. 첫째 수술 전에 1-2회의 TPF 화학치료 를 선행하였고, 둘째 수술 뒤에 1-4 cycle의 화학치료와 방사선치료를 받았다. 세번째 완벽한 종양절제와 많은 복원술의 방법에 기인한다. 또한 T3-T4, 나쁜 세포의 분화도, 림프절의 침범 등이 중요한 요인으로 본다. 또한 복원술과 화학치료 방사선 치료가 재발을 낮출 수 있다고 본다.
Identifying relevant factors of tumor recurrence can help establish treatment standards. Surgery remains the preferred treatment for OSCC. However, for patients at T3-T4 stages and with poorly differentiated tumors, primary tumor resection margin should be expanded, generally 2 cm or more from the tumor, to ensure surgical safety. Flap repair should also be performed. Our results showed that the application of flap repair significantly reduced local tumor recurrence. de Vicente et al.[6] have followed up 98 patients with OSCC. They found that the mortality was 47.0% in patients with flap repair and was 67.3% in patients without flap repair (P < 0.05). Therefore, the application of free flap repair can improve the 5-year survival rate of patients. In addition, neck lymph nodes should be carefully cleaned while resecting the primary tumor. For patients with cN0 diseases, lymph nodes in the ipsilateral neck I-III regions should be selectively cleaned. Capote et al.[7] have performed selective neck lymph node dissection on pT1N0M0 patients and primary tumor resection on patients with pT2N0M0 tumors. They found that the regional recurrence rate was significantly lower in patients who underwent selective neck lymph node dissection than in those who underwent primary tumor resection only. Thus, neck lymph node dissection is an important prognostic factor for the recurrence of OSCC. For neck lymph node-positive patients, radical neck dissection should be performed in the ipsilateral carotid I-V region. Because OSCC might migrate to the IIb region, the sternocleidomastoid should be removed during surgery. Preoperative neoadjuvant chemotherapy and postoperative adjuvant chemotherapy or radiotherapy can also reduce recurrence and improve prognosis. All patients in this study underwent 1-2 cycles of preoperative neoadjuvant chemotherapy, and patients in advanced stages were treated with 4 cycles of adjuvant chemotherapy or radiotherapy after surgery. The recurrence rate was 32.7%, and the 5-year survival rate was 54.5%, both of which were satisfactory. Cooper et al.[8] have also reported that postoperative radiotherapy and chemotherapy can improve disease-free survival and improve local and regional control rate in patients with head and neck squamous cell carcinoma. López Rodríguez et al.[9] have reported that preoperative radiotherapy and chemotherapy for head and neck squamous cell carcinoma at N2-N3 stage can completely control neck lymph node metastasis and achieve local and regional effectiveness.
In this study, we explored clinicopathologic factors of recurrence in OSCC and discussed some perspectives for clinical reference. In recent years, the expression of certain genes has been reported to closely relate to the recurrence of OSCC. Cheng et al.[10] have reported that serum placental growth factor (PIGF) level could be used as a biomarker to predict the therapeutic effect on OSCC, as well as its recurrence and prognosis. Liu et al.[11] have reported that vimentin up-regulation and E-cadherin and β-catenin down-regulation were associated with recurrence and survival of OSCC patients. Therefore, our future work will explore mechanisms of OSCC recurrence at the molecular level to develop better treatment strategies.

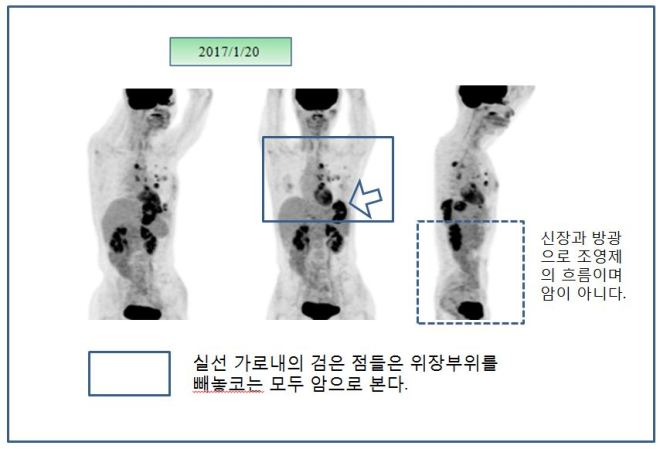
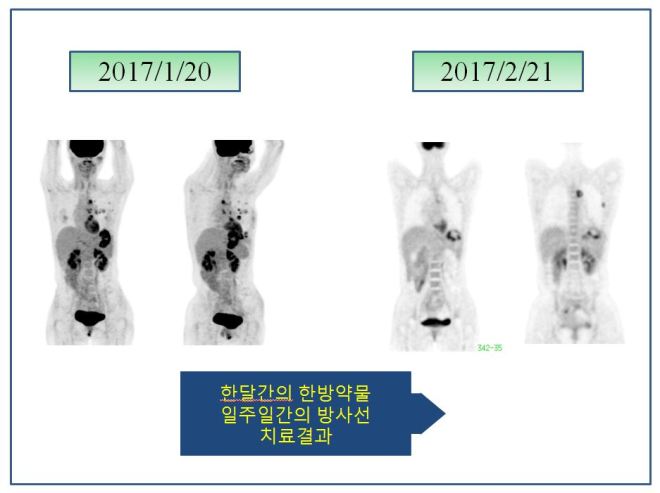
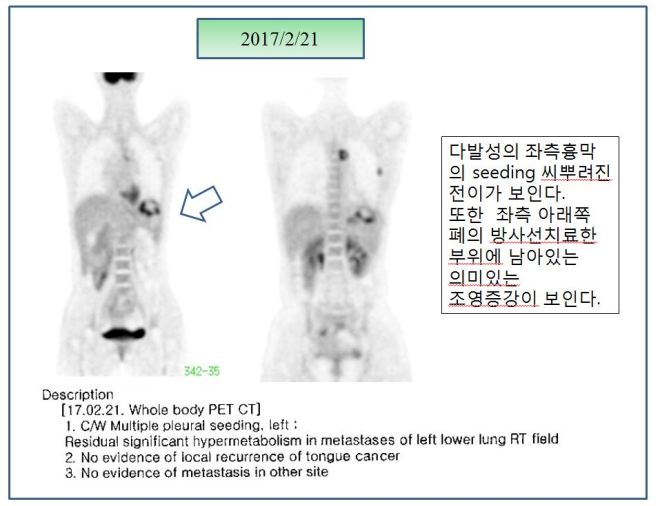 위의 설명대로 아직은 좌측 옆구리에 검은 점들로 보여지는 seeding nodules이 남아 있고 종격동 부위에도 보이지만 이는 SUVmax가 낮아서 언급이 안 되었고 사진상 보이는 것처럼 현저한 치료 전과 후의 차이를 보이고 있다. 이전 폐와 mammary lymph node들에 보이던 음영이 현저히 사라져 소실되었다. 그래서 단지 좌측 폐의 하엽 부위만이 소견서에 언급되었다.
위의 설명대로 아직은 좌측 옆구리에 검은 점들로 보여지는 seeding nodules이 남아 있고 종격동 부위에도 보이지만 이는 SUVmax가 낮아서 언급이 안 되었고 사진상 보이는 것처럼 현저한 치료 전과 후의 차이를 보이고 있다. 이전 폐와 mammary lymph node들에 보이던 음영이 현저히 사라져 소실되었다. 그래서 단지 좌측 폐의 하엽 부위만이 소견서에 언급되었다.