Today’s case is about a patient with glioblastoma (GBM), the most aggressive WHO Grade 4 brain tumor.
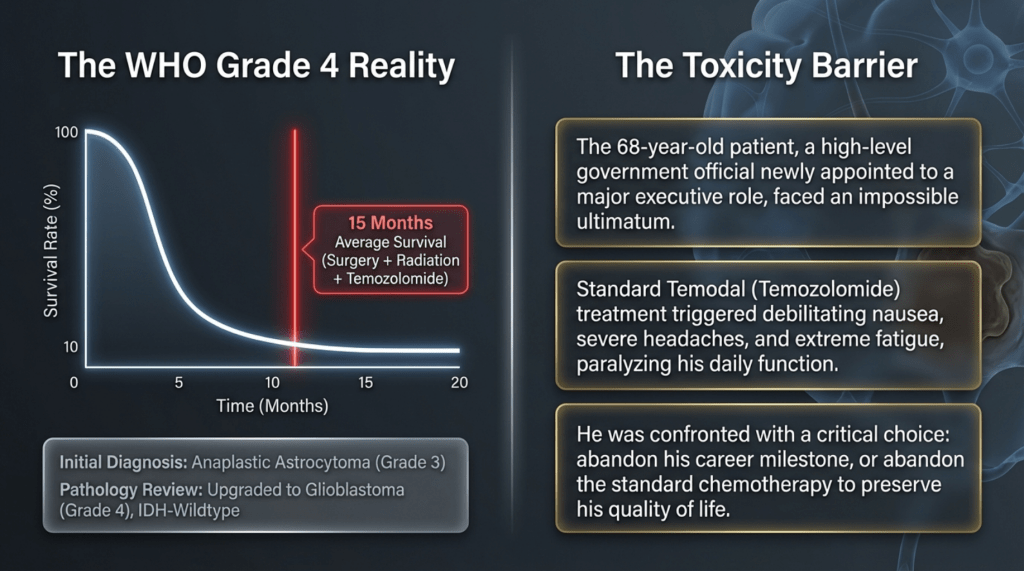
Initially, the patient was diagnosed at Chungnam National University Hospital with anaplastic astrocytoma (AA, WHO Grade 3). However, after being transferred to Seoul National University Hospital, an external slide review was conducted and the histopathology was reassessed.
Based on this review, the final diagnosis was revised to:
Glioblastoma (GBM), IDH-wildtype, WHO Grade 4.
As shown in the data below, this patient’s pathology corresponds to the subtype with the poorest prognosis, with a currently known median overall survival of approximately 15 months.
Reference)
Highest Grade and Glioblastoma (Grade 4)
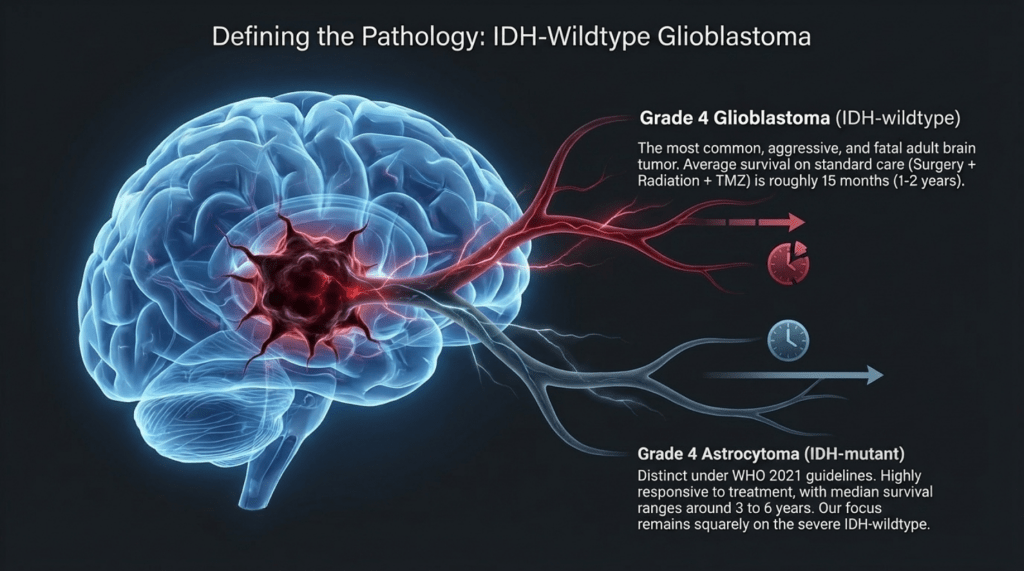
🔴 Grade 4: Glioblastoma (IDH-wildtype)
Verification: Accurate. This is the most common and most aggressive primary brain tumor in adults. With standard treatment (surgery + radiotherapy + temozolomide), the median overall survival is approximately 15 months (generally within a range of 1–2 years).
🔴 Grade 4: Astrocytoma (IDH-mutant, Grade 4)
Verification: Accurate. In the past, this entity was considered part of glioblastoma; however, according to the WHO 2021 classification, tumors with an IDH mutation are now classified separately as “Astrocytoma, Grade 4.”
Compared to glioblastoma (IDH-wildtype), it shows a significantly better response to treatment, with a median survival of around 3 years (reported in recent studies to range approximately 3–6 years).
After receiving the initial diagnosis, the patient, recognizing the highly aggressive nature of the disease, reportedly began to put his personal affairs in order.
During the course of standard treatment—including surgery, radiotherapy, and one month of temozolomide—the patient experienced severe headaches and profound side effects that led to extreme physical debilitation. As a result, he discontinued treatment and, upon the recommendation of friends, came to seek my care.
Temozolomide is typically administered for one week per month. However, the patient reported that after taking the medication in the morning, he experienced such severe nausea and vomiting that it significantly interfered with his ability to carry out daily activities.
At the time, he had just taken on an important national-level responsibility and had been in that role for a little over a year. He felt that if he continued taking the medication, his physical condition would deteriorate to the point that he would have to resign from his position immediately.
With the determination to fulfill his final duty, he decided to discontinue the medication and came to me for treatment.
Subsequently, he successfully survived beyond five years, continued to perform his duties without interruption, and ultimately completed his term and retired honorably at the standard retirement age.
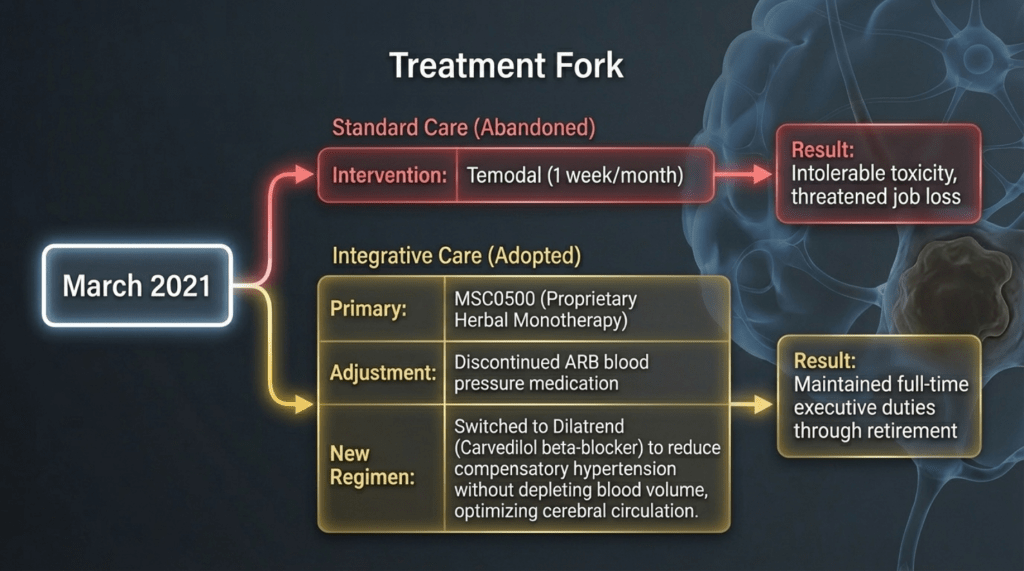
As he was both my high school and university classmate, he readily accepted my medical perspective, and treatment was initiated in March 2021.
At my recommendation, among his conventional medications, his antihypertensive therapy was adjusted. He had initially been taking an ARB (angiotensin receptor blocker), but considering his constitutional type, I determined that it was not appropriate. Therefore, it was changed to a beta-blocker (Dilatrend, carvedilol), which I considered more suitable.
With this adjustment, along with herbal medicine alone, he has now surpassed five years without recurrence and continues to lead a normal, healthy life..
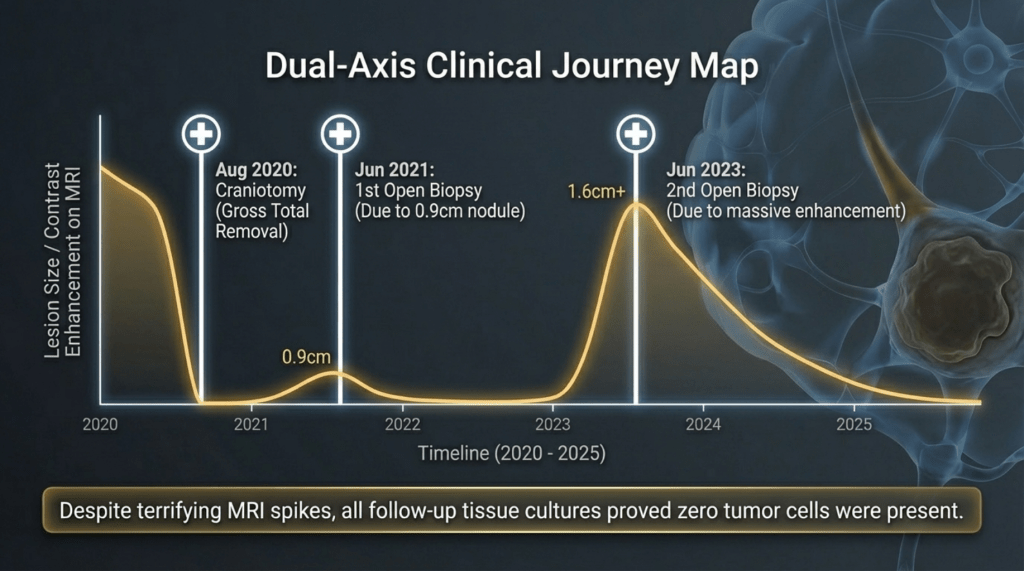
The attending physician in charge of this patient consistently maintained, at every three-month follow-up visit at Seoul National University Hospital, that “the tumor cannot simply stop growing; it is just not visible at the moment.” Based on this concern, the patient underwent two additional craniotomies for tissue sampling. However, in both cases, the pathology revealed only inflammatory changes, with no evidence of tumor recurrence.
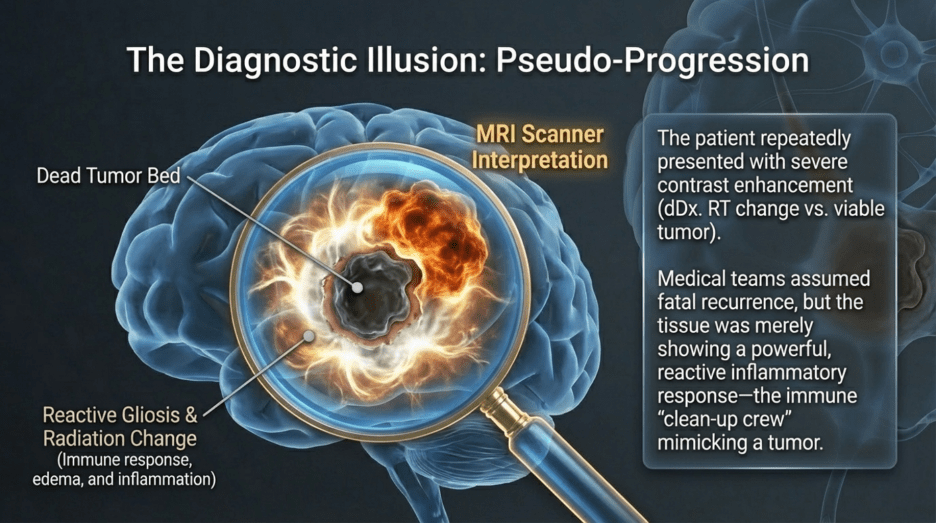
When MRI scans showed increased contrast enhancement at the surgical site, it was strongly suspected to represent recurrence. Consequently, repeat craniotomy and tissue biopsy were performed. Yet again, both instances were ultimately identified as post-radiation effects and inflammatory responses, rather than viable tumor tissue.
I have encountered several similar cases among my patients. In some instances, subtle radiologic “progression” on MRI led to recommendations for temozolomide treatment despite my advice to the contrary. Unfortunately, a number of those patients deteriorated rapidly and passed away within a few months. At that time, there were differing interpretations among physicians—some radiologists considered the findings to be radiation-induced changes, while treating physicians often interpreted them as tumor recurrence, leading to the use of temozolomide and, in my observation, rapid clinical decline.
Similarly, bevacizumab (Avastin), which is currently used in such cases, may not always be beneficial depending on the patient’s constitutional characteristics. I have observed cases with identical pathology where its use was associated with rapid worsening; I will address this issue further when discussing those cases separately.
In this particular case, the attending physician, based on extensive lifetime experience, remained convinced that the MRI enhancement represented recurrence. However, despite this expectation, no recurrence was observed throughout the remainder of the physician’s career, and the patient remained stable until the physician’s retirement.
Even as a senior professor at Seoul National University Hospital, the physician appeared perplexed and concerned during follow-up visits, expecting recurrence that never materialized. After the physician’s retirement, care was transferred to another doctor, and the patient continued follow-up for an additional two years. The imaging interval was gradually extended from every three months to every six months, and now, more than five years later, the patient remains recurrence-free.
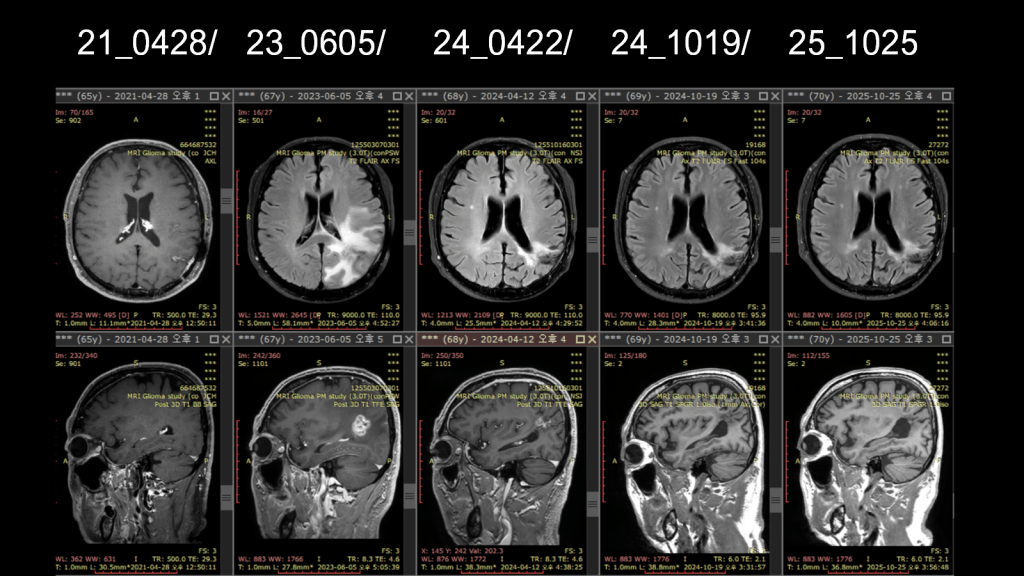
Subsequent additional biopsies performed in 2021 and 2023 confirmed that the findings were not tumor recurrence, but rather reactive gliosis and radiation-induced changes. At the time, MRI showed areas of increased contrast enhancement, which raised suspicion for recurrence. The clinical course can be summarized chronologically as follows:
1) August 2020 – 2021
Following the initial surgery in 2020, interval imaging in 2021 (and later again in 2023) demonstrated enlargement of the lesion, raising strong suspicion of tumor recurrence.
As a result, the patient underwent two additional craniotomies with tissue biopsy and culture. However, in both instances, the pathological findings revealed inflammatory changes secondary to post-radiation effects, rather than recurrent tumor.
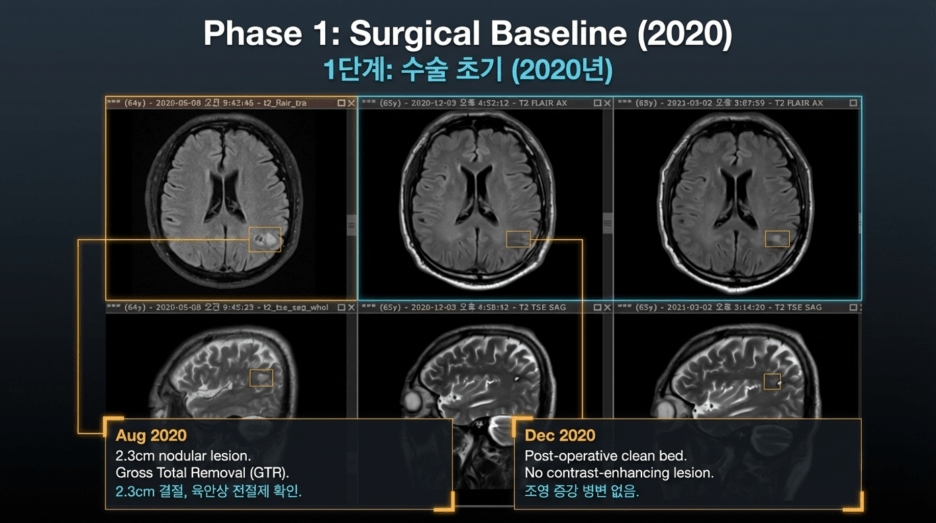
2020: Initial Onset and Surgical Course
2020-07-28: Brain MRI
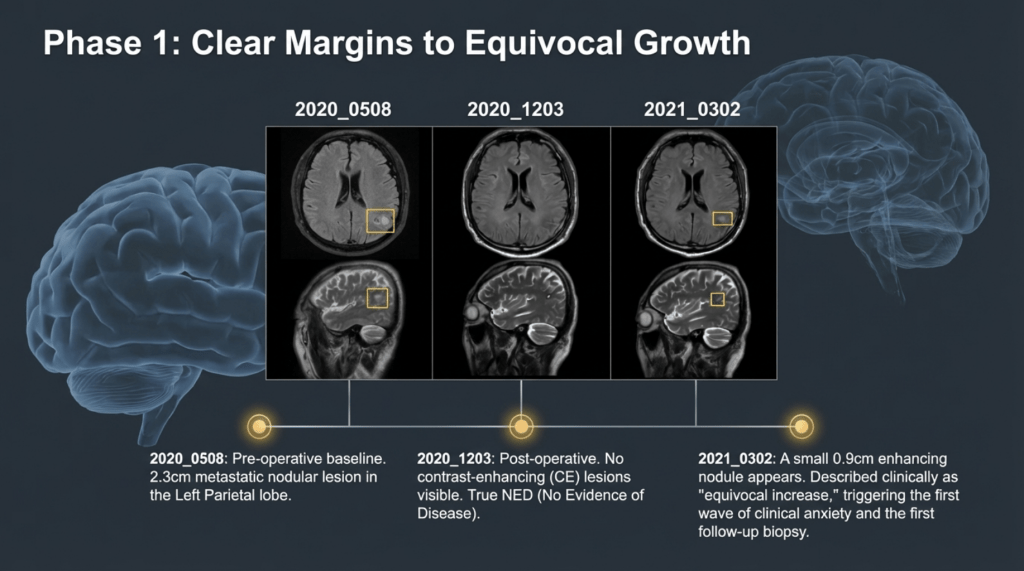
A nodular lesion measuring approximately 2.3 cm with T2 signal intensity was observed in the left parietal lobe.
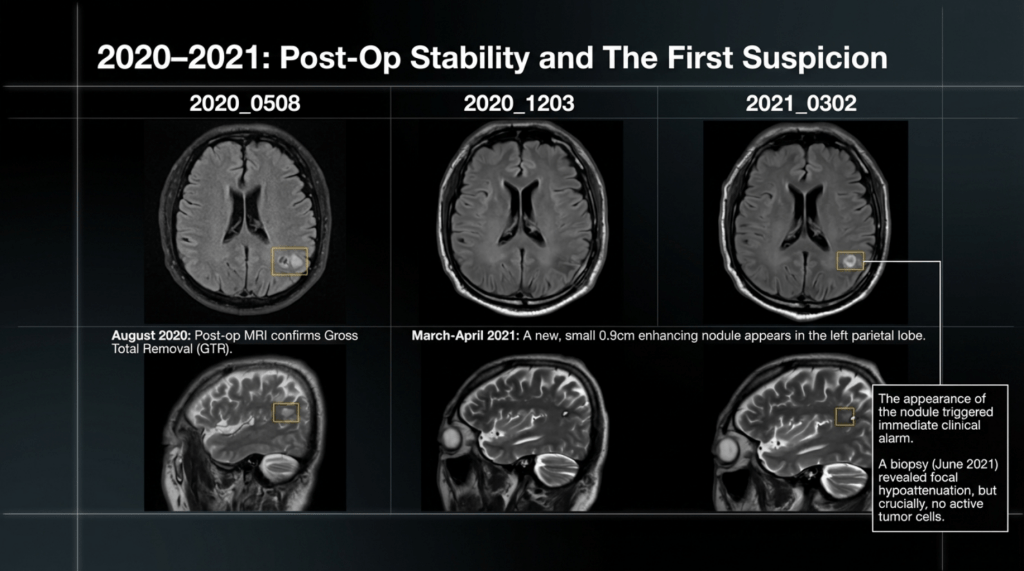
2020-08-07: Brain MRI (Postoperative)
Findings indicated gross total resection (GTR) of the mass, along with expected postoperative changes at the surgical site.
2020-12-03: Brain MRI
No contrast-enhancing (CE) lesion was identified, suggesting no radiologic evidence of residual or recurrent tumor at that time.
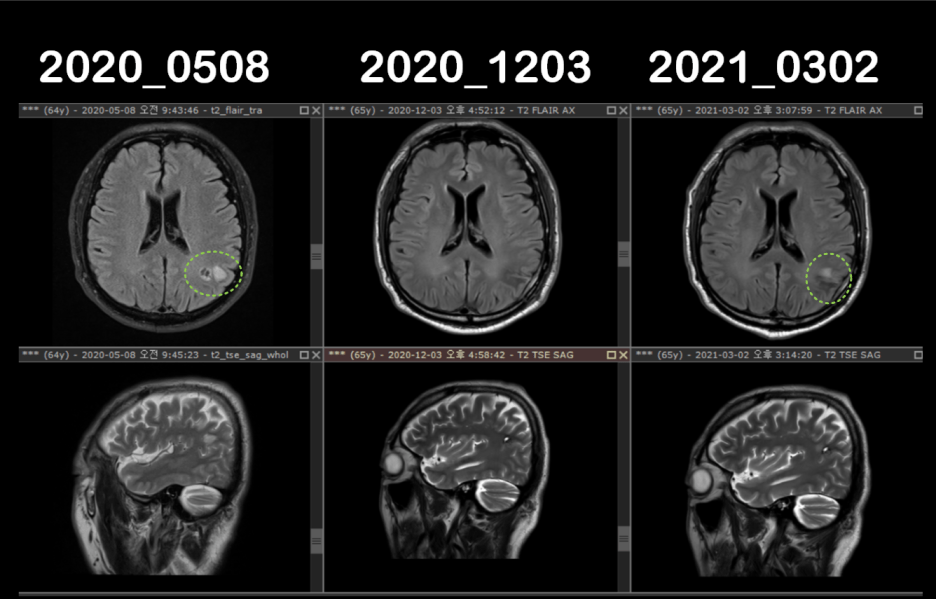
2021: Subtle Lesion and First Biopsy
2021-03-02: Brain MRI
A small nodule was observed in the left parietal lobe.
2021-04-28: Brain MRI
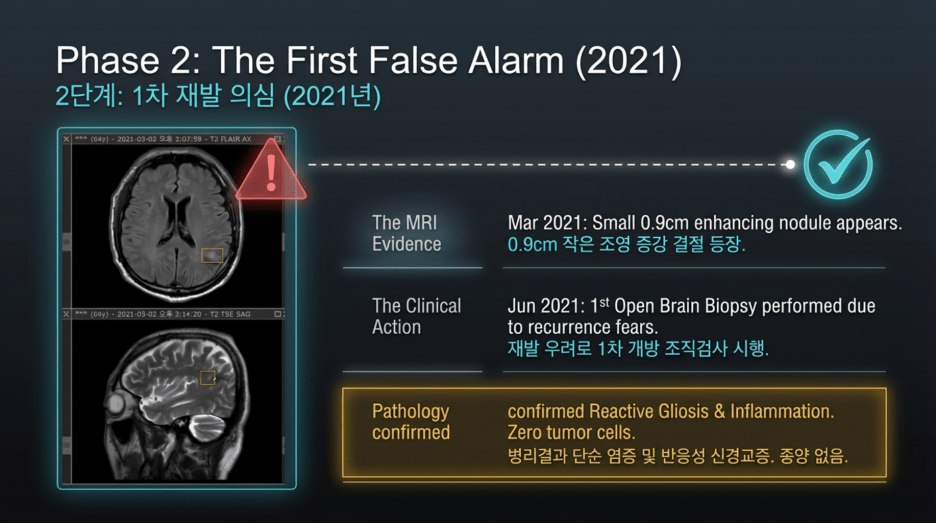
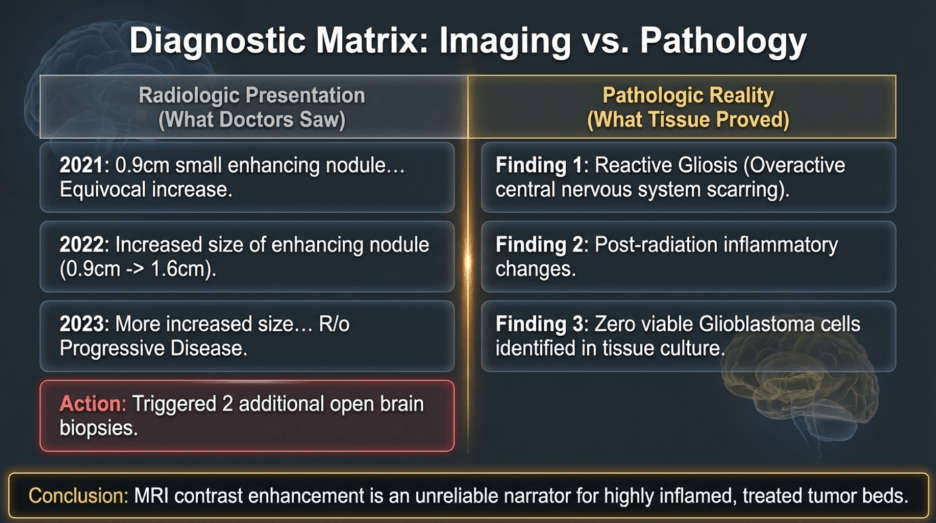
A small enhancing nodule measuring approximately 0.9 cm was identified in the left parietal lobe.
The interval change was described as equivocal, meaning that definite progression could not be clearly determined.
2021-06-02: Brain CT (After 1st Biopsy)
Status post open biopsy (S/P open Bx.). A focal hypoattenuated lesion was observed in the left parietal lobe.
2021-07-04: Brain MRI
There was no significant interval change in the previously noted ~0.9 cm enhancing nodule in the left parietal lobe.
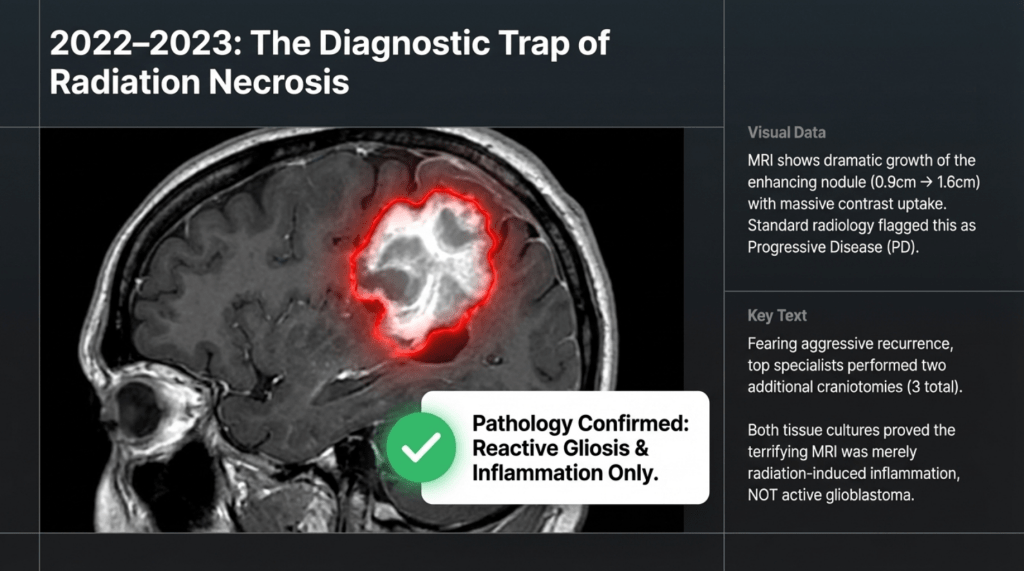
Following the first biopsy in June 2021, a second biopsy was performed in June 2023, two years later, due to radiologic concern on MRI. However, despite the markedly increased contrast enhancement seen on imaging, the lesion was ultimately confirmed to represent inflammation and edema, not tumor recurrence.
At that time, although the MRI findings appeared worrisome, I reassured the patient that this was inflammatory in nature and not indicative of recurrence. Based on my clinical experience, I strongly advised against the use of temozolomide in this situation.
The patient, by nature, was someone who, once convinced, remained steadfast in his decision. In contrast, some individuals tend to remain anxious and continuously seek alternative options even when the condition is stable. In this case, the patient maintained his course of treatment with consistency and trust.
A biopsy was performed in June 2021, and again in June 2023, during which the skull was reopened for tissue sampling. However, both times, the results showed only inflammatory changes, with no evidence of tumor recurrence. In total, the patient underwent a third craniotomy.
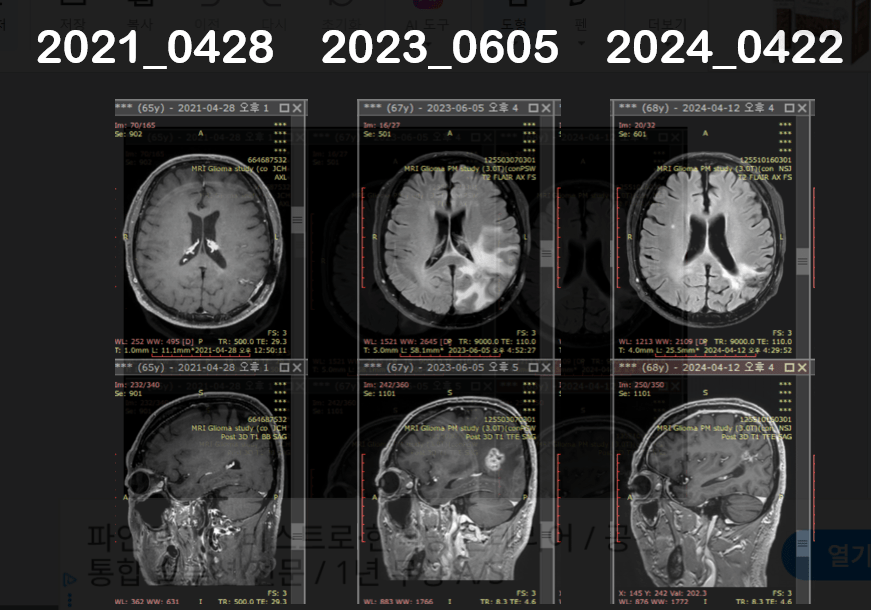
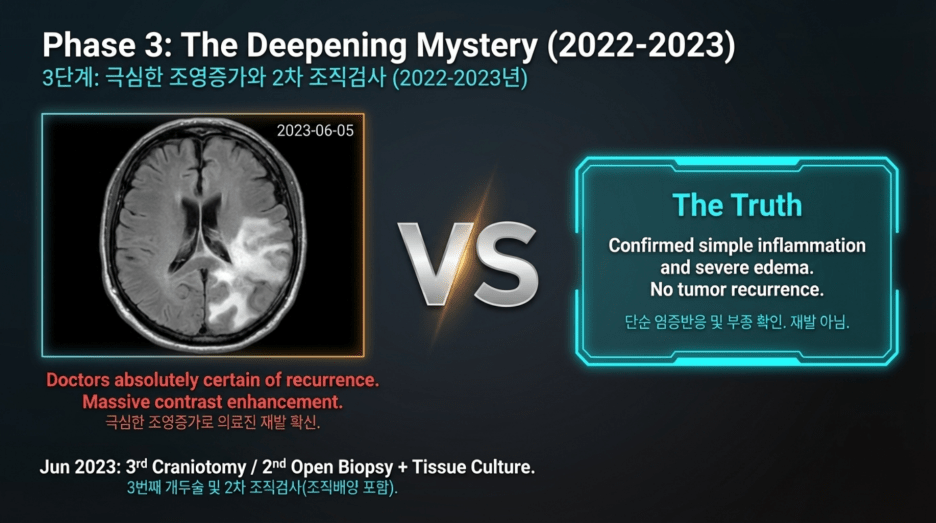
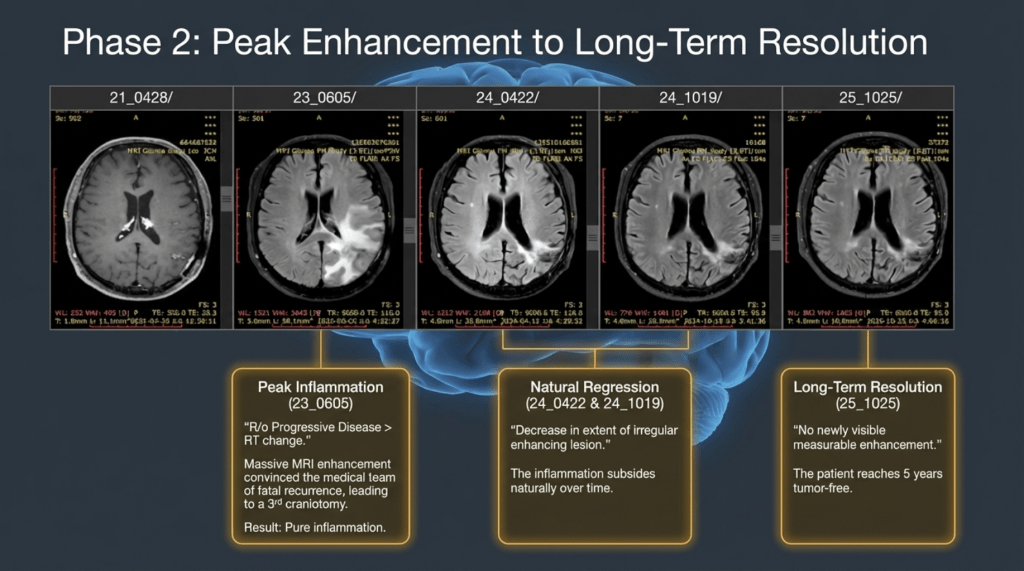
As seen in the June 2023 imaging, there was a marked increase in contrast enhancement, which at the time was strongly interpreted as definite tumor recurrence, leading to the decision to proceed with another craniotomy.
However, the final results once again demonstrated only inflammatory response, with no tumor cells identified. It is reported that even tissue culture was performed, further confirming the absence of recurrent tumor.
2022 – 2023: Lesion Progression and Second Biopsy
2022-01-21: Brain MRI
There was an increase in size of the enhancing nodule from 0.9 cm to 1.6 cm.
Differential diagnosis included radiation treatment–related change vs. viable tumor (recurrence).
2023-06-05: Brain MRI
The enhancing nodule showed further increase in size.
Findings were interpreted as more suggestive of progressive disease (PD) rather than radiation-related change.
2023-06-19: Brain CT (Post–Second Biopsy)
Status post open brain biopsy.
There were no unusual postoperative findings.
2023-10-07: Brain MRI
Findings showed an equivocal change.
The impression favored treatment-related changes (e.g., radiation effect) over tumor recurrence.
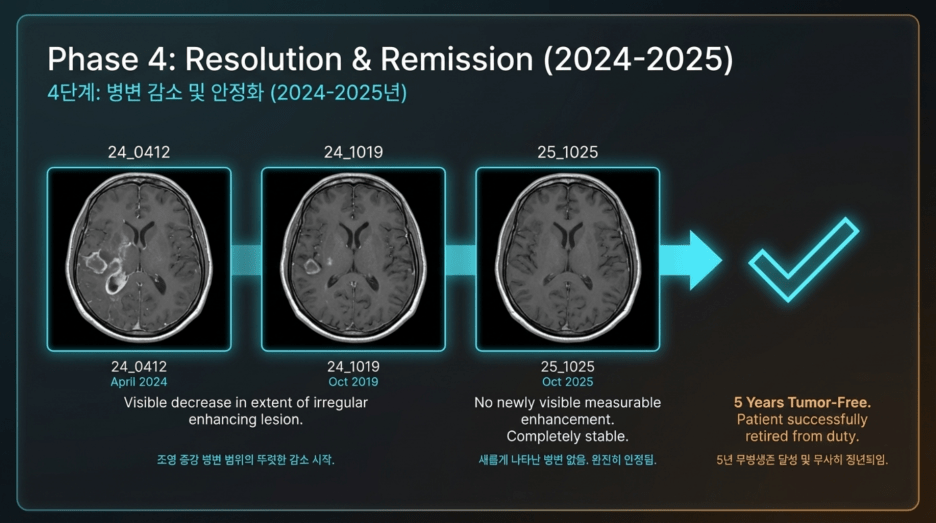
3) 2024–2025: Stabilization and Recovery Phase
During this period, there was a clear reduction in disease-related findings, and the patient successfully reached retirement. After retiring, the patient has been living well, enjoying exercise, hiking, and travel. Herbal medicine is still being continued, with a recommendation to maintain it for another 1–2 years.
Based on my clinical experience, I have observed cases where recurrence occurred even after 6–7 years. These patients had strictly adhered to dietary restrictions during treatment, but once they considered themselves cured, they began consuming previously restricted foods—such as pork, squid, octopus, and other “yang-type” foods—without control for several months, which led to recurrence.
Once recurrence occurs, treatment may prolong survival, but achieving a complete cure becomes difficult. Therefore, based on these experiences, I recommend continuing medication for approximately 7 years. Patients who remain recurrence-free during this period are more likely to achieve complete recovery and continue to live well thereafter..
Brain MRI Follow-up Summary (2024–2025)
April 12, 2024 – Brain MRI
Decrease in the extent of the irregular enhancing lesion in the left parietal lobe.
October 19, 2024 – Brain MRI
Further decrease in the extent of the irregular enhancing lesion.
April 26, 2025 – Brain MRI
Continued decrease in lesion extent. Findings are more suggestive of treatment-related changes rather than tumor recurrence.
October 25, 2025 – Brain MRI (Latest)
No newly visible measurable enhancement. No change (NC) in the extent of the pre-existing irregular enhancing lesion, indicating a stable condition.
Clinical Course Summary
The patient showed an increase in lesion size on imaging studies in 2021 and again in 2023, raising suspicion of recurrence. However, in both instances, repeat biopsies confirmed that these changes were not due to tumor recurrence but rather treatment-related (radiation-induced) effects.
Since 2024, the lesion has continuously decreased or remained stable, maintaining a status consistent with NED (No Evidence of Disease). The patient has been living a normal daily life up to the present time.
https://pubmed.ncbi.nlm.nih.gov/25359730/
A paper published by Dr. Gi Ming Lai of Daebuk University in collaboration with the National Cancer Center of Taiwan reports on a study of our institution’s compound, MSC0500. The study elucidates the mechanism by which my herbal medicine inhibits cancer stem cells in glioblastoma, and additionally includes my clinical case.

